What is SAM?
According to UNICEF, ‘Severe Acute Malnutrition (SAM) is the most extreme and visible form of undernutrition.’
SAM is a condition where the Weight for Height is -3 Standard Deviation. Children with this condition have very low weight for their height and severe muscle wasting. They may also have nutritional oedema – characterized by swollen feet, face and limbs. About two thirds of these children live in Asia and almost one third live in Africa.
Severe acute malnutrition is a major cause of death in children under 5, and its prevention and treatment are critical to child survival and development.
What are the causes of SAM?
- Poor access to appropriate, timely and affordable health care
- Inadequate caring and feeding practices, which includes lack of exclusive breastfeeding or low quantity and quality of complementary food
- Poor food security, which means an ongoing lack of food quantity and diversity, characterized in many resource-poor settings by a monotonous diet with low nutrient density, together with inadequate knowledge of patterns of food storage, preparation and consumption
- Low knowledge about food storage, preparation and consumption
- Lack of a sanitary environment, including access to safe water, sanitation and hygiene services
What is the current process of dealing with SAM in India?
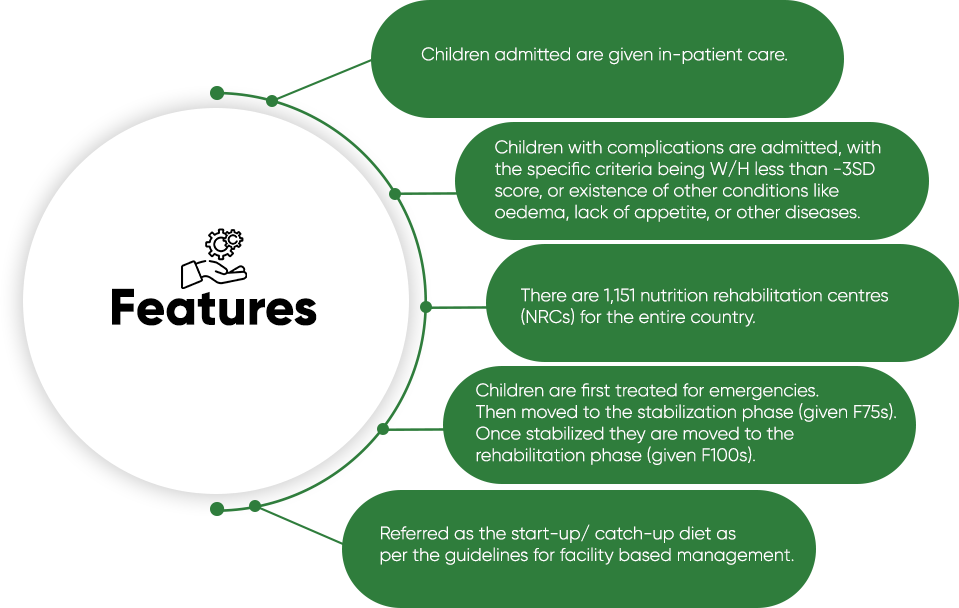
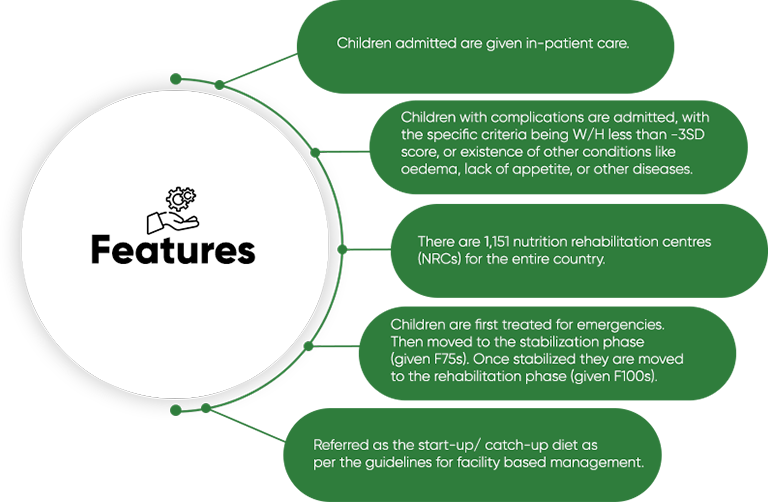
F-SAM
In India, Nutritional Rehabilitation Centres (NRCs) are the main operational method to deal with SAM at the government level, at present. This way of treating SAM children is also known as facility-based management of acute malnutrition. F-SAM is basically meant for SAM children with complications, which means only a fraction of the children become eligible for this process.
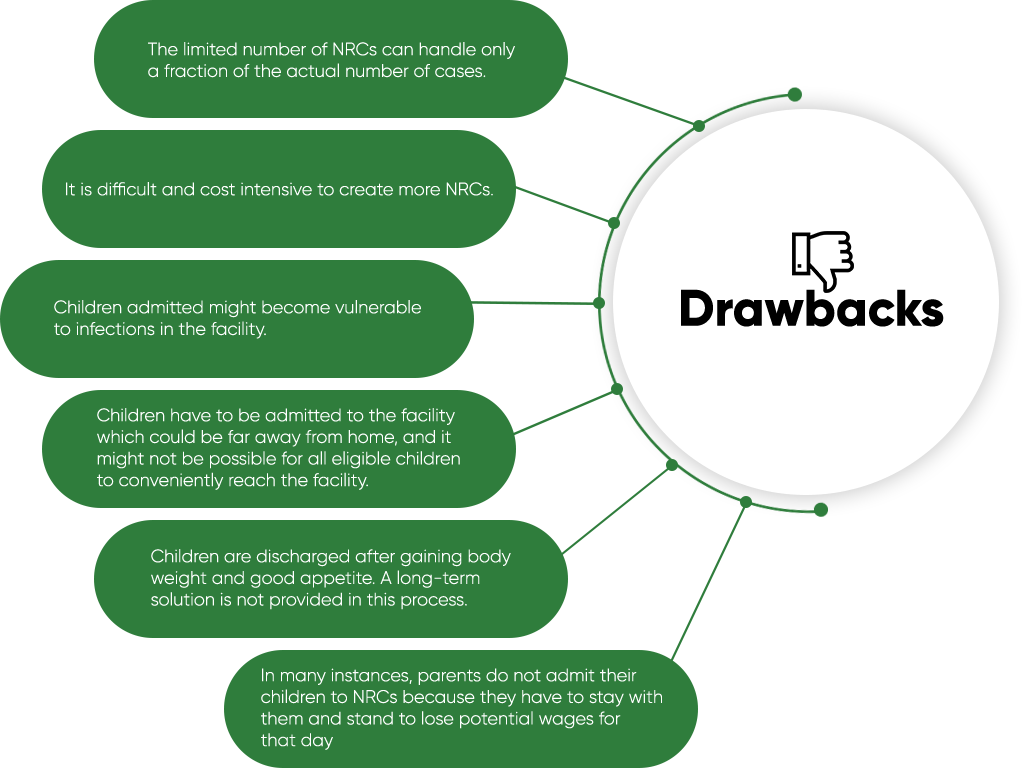
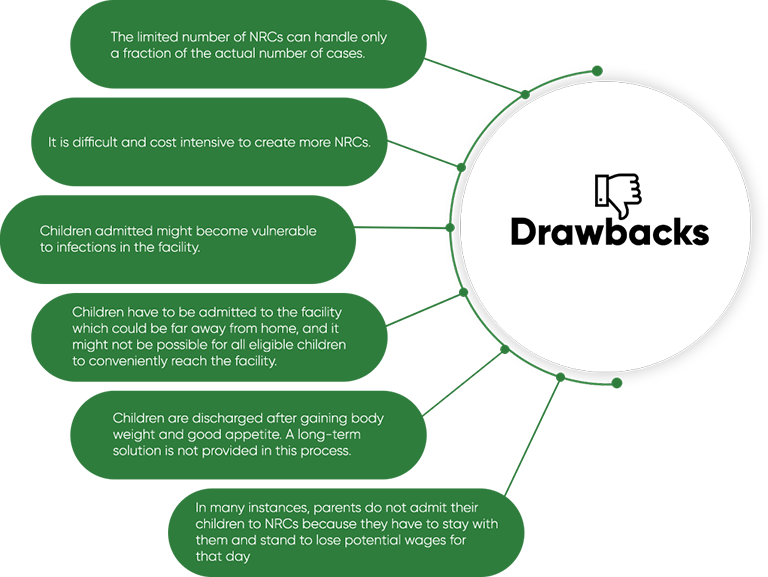
What is the proposed solution?
At present, there is no substantial process for treating children with a lesser degree of severity, which is where a community-based approach to SAM or CMAM can be introduced. CMAM is meant for SAM children without any complications, which means that about 85-90% of the children can come into this fold.
Both UNICEF and WHO prescribe CMAM as the treatment protocol for SAM.
Here are some primary features of CMAM:
- Approximately 85-90% of children with severe wasting do not have medical complications and can be managed safely through CMAM.
- CMAM can be implemented through as many Anganwadis as present under the ICDS system. New structures are not required to be built.
- It proposes an in-built response mechanism through frontline health workers and mothers.
- It strengthens the already existing community-based framework, making it a cost effective process.
- Under CMAM, children can receive continuity of care after discharge.
- This process also reduces the exposure to hospital acquired infections.
CMAM is by no means a replacement of NRCs, but a fortification of the existing process that can eventually result in covering the maximum number of affected children.